-
Credits
- Section Writer: Dr. Om J Lakhani
- Section Editor: Dr. Om J Lakhani
-
Q. What is the mortality with thyroid storm?
- 10-30%
-
Q. Thyroid storm only occurs in Graves disease, True or false?
- False
- It can occur in any cause of hyperthyroidism
-
Q. What are the precipitating factors?
- Thyroid surgery
- Non-thyroid surgery
- Parturition
- Iodine load
- Trauma
- Infection
- Sudden discontinuation of thyroid medications
-
**Clinical features **
-
Q. Which system is predominantly involved?
- CVS
-
Q. What are the CVS manifestations?
- HR >140 bpm
- Atrial fibrillation
- Hypotension
- Congestive heart failure
-
Q. What are the neurological manifestations?
- Agitation
- Delirium
- Psychosis
- Stupor
- Coma
-
Q. What is the importance of CNS manifestations?
- Some say CNS manifestations are essential for distinguishing thyroid storm from otherwise compensated hyperthyroidism
-
Q. What are the GI manifestations?
- Abdominal pain
- Diarrhea
- Nausea and vomiting
- Liver failure and jaundice
-
Q. What are the physical examination findings?
- Same as hyperthyroidism
- Hyperpyrexia may be noted – in temperature of 104 to 106 degree F
-
**Lab features **
-
Q. Apart from the TFT, which are the other lab abnormalities noted?
- Abnormal LFT
- Leukocytosis or leukopenia
- Hypercalcemia
- Hyperglycemia
-
Q. What is the cause for hyperglycemia?
- Catecholamine induced:
- Inhibition of insulin release
- Increase glycogen breakdown
- Catecholamine induced:
-
Q. What is the cause of hypercalcemia?
- Hemoconcentration
- Increased bone resorption
-
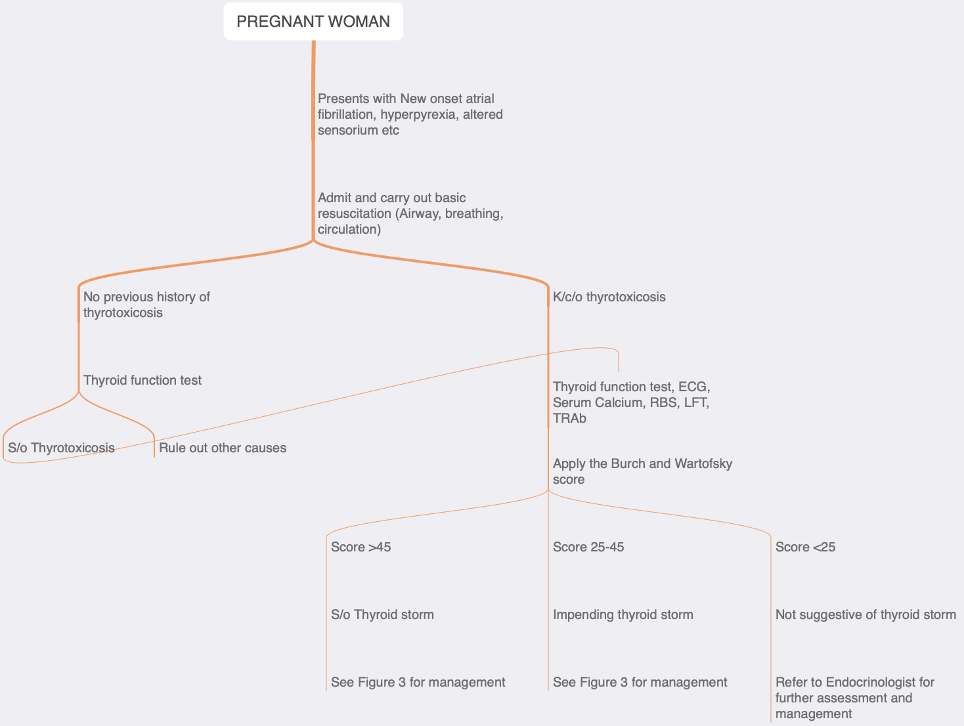
Q. What is the name of diagnostic criteria used for diagnosis of thyroid storm?
- Burch and Wartofsky’s criteria
-
Q. What are the components of these criteria?
-
Temperature
- 99 to 99.9 - 5
- 100-100.9- 10
- 101-101.9-15
- 102- 102.9 – 20
- 103-103.9- 25
- ≥ 104 – 30
-
CVS
- Tachycardia
- 99-109- 5
- 110-119 – 10
- 120-129-15
- 130-139-20
- ≥ 140 – 25
- Atrial fibrillation- 10
- Heart failure
- Mild- pedal edema- 5
- Moderate – bibasilar crepts – 10
- Severe- pulmonary edema- 15
- Tachycardia
-
GIT
- Moderate – 10
- Abdominal pain
- Nausea/vomiting
- Diarrhea
- Severe- liver failure- 20
- Moderate – 10
-
CNS
- Mild- agitation – 10
- Moderate- delirium, psychosis- 20
- Severe- stupor, coma- 30
-
Precipitating event
- Negative- 0
- Positive- 10
-
Q. What is the interpretation of the total score?
- <25- thyroid storm unlikely
- 25-44- support diagnosis
- ≥ 45 = thyroid storm
-
Q. What is the problem with these criteria?
- They are sensitive but not specific
-
Q. Is the degree of hyperthyroidism a criterion for thyroid storm?
- No
-
Q. Apart from the above score, which is another score that is used for thyroid storm?
- Akamizu criteria
-
Q. Describe the Akamizu criteria ?
-
Akamizu criteria are more specific but less sensitive
-
TS1- thyroid storm grade I
- First combination
- Thyrotoxicosis +
- CNS manifestation +
- Plus one or more of GIT, CVS, or fever
- Alternate combination
- Thyrotoxicosis + 3 or more of GIT, CVS, and fever
- First combination
-
TS2
- First combination
- Thyrotoxicosis + 2 or more of the above combinations (Except CNS)
- Alternate combination
- Similar to TS1 first combination but t3, t4 not available at present, but the patient has a history of thyrotoxicosis from the previous report
- First combination
-
-
**Treatment **
-
Q. Summarize the timing of medications in the management of thyroid storm as described by AACE guidelines
- Timing
- PTU, Cholestyramine, Methimazole (20 mg /4 hrly), and Propranolol- 4 hourly
- SSKI- 6 hrly
- Hydrocortisone – 8 hrly
- Timing
-
Q. What is the first step in the management of thyroid storm?
- Propranolol – 60-80 mg every 4-6 hours
- Adjusted according to heart rate and blood pressure
- Alternate drug is esmolol
-
Q. What is the role of beta-blockers?
- Reduced HR
- Reduced adrenergic symptoms
- At high doses impairs T4 to T3 conversion
-
Q. Which antithyroid drug is preferred in thyroid storm?
- PTU
- Because it also blocks T4 to T3 conversion
- Dose is 500 mg -1000 mg loading dose followed by 200 mg every 4 hourly (guidelines say 250 mg)
-
Q. What is an alternate to PTU?
- Methimazole
- Given 20 mg every 4 hourly
-
Q. What is done 1 hour after ATD is administered ?
- Iodine is given
- SSKI- 5 drops 6 hourly or
- Lugol’s – 10 drops 8 hourly
- Iodine is given
-
Q. What is the role of iodine?
- Blocks new hormone synthesis
- Blocks release of thyroid hormone
-
Q. Why is it given 1 hour after ATD?
- To prevent iodine from being used as a substrate for thyroid hormone synthesis
-
Q. What is the role and dose of hydrocortisone?
- Hydrocortisone – 300 mg stat followed by 100 mg IV / 8hrly
- Rationale
- Treat subclinical adrenal insufficiency
- Block t4 to t3 conversion
- Dexamethasone can be an alternative
-
Q. What is the role of bile acid sequestrants?
- Cholestyramine is given in a dose of 4 gram every 4 times a day
- It reduces enterohepatic circulation of thyroid hormone
- It is available as CHOLTRAN powder for oral soln in a dose of 4 grams
-
Q. What antipyretic is preferred in thyroid storm?
- Acetaminophen and not aspirin
-
Q. Why not aspirin (salicylates)?
- Asporin (salicylates) prevents binding of t3 and t4 to TBG hence increases the free hormone level
- Salicylates increase metabolic rate
-
Q. Which are other measures?
- Treat the precipitating cause, especially infection
- Correct fluid deficit- remember patient may have CCF, so be careful
- Diuretics may be needed in CCF
- Drugs may have to be given via RT if the patient has altered mentation
-
Q. Can beta blocker be given IV?
- Yes
- Propranolol 1 mg/kg over 10 min - repeat very 4-6 hours
- Metoprolol can also be given IV
- Esmolol is given 250-500 mcg/kg loading dose followed by infusion of 100 mcg/kg/min
- #Clinicalpearl
- ATD blocks new thyroid hormone synthesis
- Hence its action has a lag time of 1-2 hours
-
Q. Which has a longer duration of action = PTU or Methimazole?
- Methimazole has a longer duration of action
-
Q. What is alternate means of giving PTU other than orally?
- It can be given as enema or suppository
- It can be given IV by dissolving it is in Normal saline made alkaline by adding sodium hydroxide
- Methimazole can also be dissolved in neutral isotonic saline and passed through 0.22 um filter
-
Q. What is done if ATD is absolutely contraindicated because of agranulocytosis or severe hepatotoxicity?
- Emergent thyroidectomy may be required
- Patient is treated with other medications for 5-7days and then taken up for surgery
-
Q. Why does iodine inhibit thyroid hormone synthesis?
- iodine blocking its uptake by NIS
- Wolf Chiakoff effect- Iodine blocking organification of Tg
-
Q. Which are other options for management?
- Plasmapheresis
- Use of iodinated contrast agent
- Lithium
-
Q. What kind of iodinated contrast is used, and what dose?
- Iopanoic acid is used
- It is used in a dose of 0.5-1 gram/day (500 mg BD)
- It is the agent used on oral cholecystography
- #Clinicalpearl
- Iodine given orally can be irritating to GIT
- Can be mixed with food or diluted in 240 ml liquid
- #Clinicalpearl
- Definitive therapy must be considered once the treatment for thyroid storm is done
-
Q. What is the iodine content in Lugol’s solution?
- 6 grams per drop (0.05 ml drop)
-
Q. What about SSKI?
- Ie 50 mg per drop (0.05ml)
-
Q. Give an outline of the management of thyroid storm in pregnancy
-
Q. Give an initial triage for pregnant women with suspected thyroid storm in pregnancy?
-
Q. Is there any guidance on obstetric management in these cases?
- There is little or no data on the management of the obstetric aspect of thyroid
storm. - The question of continuing the pregnancy should be decided based on
individual cases. - It must be kept in mind that thyroid storm is a potentially
life-threatening condition of the mother
- There is little or no data on the management of the obstetric aspect of thyroid
-
Q. Where can I read more about the thyroid storm in pregnancy?
- Please see our article in the AOGD journal . Click the link below:
- {{pdf: https://firebasestorage.googleapis.com/v0/b/firescript-577a2.appspot.com/o/imgs%2Fapp%2FMedical_learning%2FSXG-f22Wc7.pdf?alt=media&token=5a0828bd-3b2a-49a0-89bc-ecc7561b1e80}}

-
Q. Can thyroid storm occur after head and neck trauma ?
- Yes
- Though rare, thyroid storm has been reported from head and neck and neck trauma including
- Assault
- Suicide attempts by hanging and accidental self-inflicted injury
- following rapid sequence intubation [1]
-
Q. Can thyroid storm present with HCG producing tumors ?
- TSH and HCG have similar structure
- Hence excess of HCG can act on TSH receptor because of specificity spillover and can cause thyrotoxicosis
- Thyroid storm has been reported after HCG producing tumors
- Recently in male a HCG producing Testicular Choriocarcinoma has been reported to cause thyroid storm [2]
-
Q. What are the factors associated with increased mortality from thyroid storm ?
- In a recent study conducted from Taiwan the following factors were associated with increased mortality [3]
- older age
- male sex
- underlying ischemic stroke
- myocardial infarction
- heart failure
- kidney disease
- atrial fibrillation
- depression
- chronic obstructive pulmonary disease
- diabetes mellitus
- cancer
- end stage renal diseases
- In a recent study conducted from Taiwan the following factors were associated with increased mortality [3]
Please consider donating to "Notes in Endocrinology" to keep us going. Please visit our DONATION page to know more
Ref: Radhi MA, Natesh B, Stimpson P, Hughes J, Vaz F, C Dwivedi R. Thyroid Storm in Head and Neck Emergency Patients. Journal of Clinical Medicine. 2020 Nov;9(11):3548 ↩︎
Ref: Martínez-Gallegos JC, Ovalle-Zavala EA. Thyroid Storm Associated with Testicular Choriocarcinoma. European Journal of Case Reports in Internal Medicine. 2020;7(10). ↩︎
Kornelius E, Chang KL, Yang YS, Huang JY, Ku MS, Lee KY, Ho SW. Epidemiology and factors associated with mortality of thyroid storm in Taiwan: a nationwide population-based study. Internal and Emergency Medicine. 2021 Apr;16(3):601-7. ↩︎