T3 (Liothyronine, Linorma T3)
Written by Dr. Om J Lakhani
If you find this useful, please use the link to see the various ways in which you can Support us →
For consultation with Dr. Om J Lakhani please see Online Consultation →
Key Information:
- Support us by purchasing our book - Click here for more details: Volume 1- THE BEST OF NOTES IN ENDOCRINOLOGY BOOK SERIES
- Support you by Becoming a YouTube member (Click here)
- For Online Consultation with a Qualified Endocrinologist, Click Here
Plain Language summary of the Article
LINORMA T3 (Liothyronine) is a prescription thyroid medication available in India in 5 mcg and 20 mcg doses. This T3 thyroid hormone supplement is primarily used for patients with hypothyroidism who have residual symptoms despite adequate T4 treatment. Dosing typically starts at 10-20 mcg every 8 hours for adults, with potential increases to 60 mcg/day in 2-3 divided doses after one week. For elderly patients and children, a lower dose of 5 mcg/day is recommended.
Key features of LINORMA T3 include:
- Fast onset of action (within hours)
- Reaches steady state in 2-3 days
- Nearly complete gastrointestinal absorption
- Half-life of 1-2 days
- Safe profile with no increased risk of atrial fibrillation, fractures, or cardiovascular disease
- For pediatric administration, the 20 mcg tablet can be dissolved in 20 ml water
In myxedema coma, LINORMA T3 is administered as 60 mcg via RT followed by 20 mcg every 8 hours. Clinical studies show T3 supplementation can improve quality of life in hypothyroid patients, though European and British guidelines recommend its use as experimental rather than routine treatment.
For combination therapy with T4, guidelines recommend a T4:T3 ratio of 13:1 to 20:1 by weight, with T3 doses split between morning and evening administration. One standard T3 dose is equivalent to three T4 doses (e.g., 100 mcg T4 = 33.3 mcg T3).
Main Notes
- Q. What is the brand of T3 (Liothyronine) available in India ?
- Linorma T3
- Q. What happens to the T3 when we treat a hypothyroidism patients with LT4 ?
- Studies in humans have shown that the use of LT4 for treating hypothyroidism leads to normalization of TSH , but abnormal FT4/F T3 ratio.
- The F T3 is not normalized like it should be because of LT4
- This is because with the use of T4 --> the TSH is normalized first before T3 can be corrected
- Q. Where are the Type 1 deiodinase and Type 2 deiodinase found in the human body?
- Type 1 deiodinase- Liver and Kidney
- Type 2 - is found in the heart, skeletal muscle, CNS, fat, thyroid, and pituitary
- Q. Of the above 2 - which contributes most to the T3 levels?
- Type 2 deiodinase contributes 80% of the T3 levels
- Q. So why does treatment with LT4 lead to pooer T4/ T3 ratio ?
- LT4 given is taken up by the hypothalamus and pituitary - converted to T3 by the local D2 and then it normalizes TSH rapidly
- However, the above correction occurs faster compared to the normalization of T3 levels in the peripheral circulation
- Hence a adequate T3 levels is never achieved in before the TSH is normalized

- Q. Which specific Type 2 deiodinase polymorphism has produced this debate ?
- Thy92 Ala
- Q. What effects of the thyroid hormone are thought to occur via a non-canonical or non-thyroid receptor pathway?
- Effect on cancer growth
- Q. What are the issues with a clinical trial with T3 /T4 combination?
- The right patients may not have been included
- The right patients include those who are dissatisfied with the T4 replacement
- Q. What is the pharmacological equivalence between T3 and T4?
- One T3 = Three T4
- ie 100 mcg of T4 = 33.3 mcg of T3
- 40 mcg of T3 = 115 mcg of T4
- Q. What are the problems with T3 assays?
- At low concentration, the T3 or F T3 immunosassays are less reliable
- It is also affected by the patient's factors
- Patients on dietery restriction have lower levels
- Patients with illness may have lower levels
- Age
- Time of the day
- Q. If given as monotherapy, how is T3 given?
- it is given three times a day
- Typically 10 mcg of TDS would be around 120 mcg of T4
- Trials have used twice a day T3 generally because of patient compliance issue
- Q. What is the half-life of T3 ?
- 22 hours
- Q. In our terms, how much thyroid hormone is produced by the thyroid gland?
- 100 mcg of T4 is produced and about 5 mcg of T3 is produced by normal thyroid gland
- This is about a 14:1 ratio
- #Clinicalpearl: Slow release T3 preprations are required to solve the problem of T3 and T4 combination
- Q. What happens to TSH with T3 monotherapy is given ?
- Studies have shown that with T3 monotherapy, the TSH levels tends to be a little lower
- Fluctuations are also more
- Lower TSH here may not represent overcorrection
- Q. Which are two key psychological outcomes attributable to hypothyroidism?
- Two outcomes attributable to hypothyroidism include
- Emotional susceptibility
- Tiredness
- Depression and Anxiety are NOT attributable to thyroid dysfunction
- Two outcomes attributable to hypothyroidism include
- Q. What is the top psychological concern of patients with hypothyroidism?
- Fatigue is the chief concern in patients with hypothyroidism
- General fatigue
- Physical fatigue
- Mental fatigue
- Fatigue is the chief concern in patients with hypothyroidism
- #Clinicalpearl
- Thyroid-related QoL indices tend to perform better compared to general QoL includes like SF-36 etc
- For fatigue specifically, thyroid-related fatigue may be different from other fatigues!
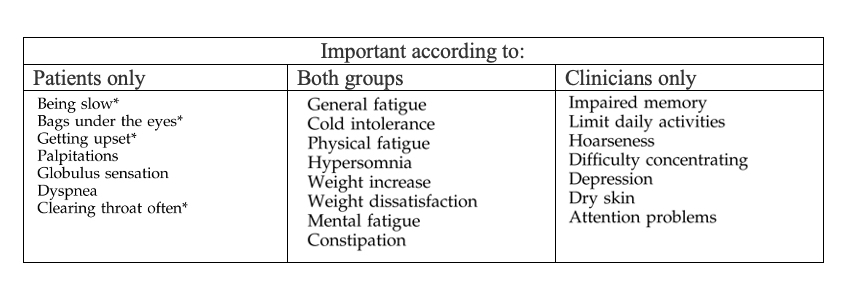
- Q. In Hypothyroidism, what is the difference between patient-perceived symptoms and clinician-perceived symptoms?
- Q. Which two tests should be done to assess tissue-level hypothyroidism and its correlation with hypothyroidism?
- lipid profile
- Creatine kinase
- They correlate with symptoms
- Q. What is the main use case for T3?
- It is to be used in patients who continue to have residual symptoms even after giving an adequate dose of T4.
- Q. How fast is the onset of action of T3?
- Within a few hours
- Q. At what time does T3 achieve a steady state?
- Over 2-3 days
- Maximum pharmacological response is seen after 2-3 days
- Q. What is its half-life?
- 1-2 days
- Q. How is it absorbed?
- It is almost completely absorbed from the GI tract
- Q. Do patients on T3 have a higher risk of treatment-related complications?
- No
- There is no evidence of increased risk of atrial fibrillation , no increased fracture risk, and no increased risk of CV disease
- Q. In studies, does T3 show improvement in quality of life?
- Yes it does
- Q. What do European and British guidelines say about T3?
- Guidelines Suggests the use of L-T3 as an experimental approach and not for routine use in patients receiving LT4
- Recommends use of L-T4 + L-T3 in a dose ratio of 13:1 and 20:1 by weight
- Recommends daily L-T3 dose to be given in two divided doses (one during breakfast and a large dose before sleeping).
- Recommends separate L-T3 and L-T4 tablets in combination therapy since available L-T4 + L-T3 combination is below the recommended dose ratio of 13:1.
- Q. Does it cross the placenta?
- No
- Q. How is Linorma T3 given in adults ?
- It is given in the starting dose of 10-20 mcg every 8 hrly
- After 1 week the dose can be increased to 60 mcg/day in 2-3 divided doses (20 mcg TDS)
- In the elderly and children 5 mcg /day is recommended
- Q. How is it used in Myxedema coma?
- 60 mcg via RT followed by 20 mcg/8hrly
- Q. Linorma T3 is available in what doses in India?
- 5 mcg and 20 mcg
- Q. How is the medication given to children?
- Dissolve the 20 mcg tablet in 20 ml of water
- Take 5 ml of the medication via syringe and give it to the patient