- Credits
- Section Writer: Dr. Om J Lakhani
- Section Editor: Dr. Om J Lakhani
Support us:
- Support us by purchasing our book - Click here for more details: Volume 1- THE BEST OF NOTES IN ENDOCRINOLOGY BOOK SERIES
- Support you by Becoming a YouTube member (Click here)
-
Q. What is the prevalence of PCOS?
- 6-10% of women in the reproductive age group have PCOS based on the original NIH criteria
-
Q. Which patients are at high risk of having PCOS?
- First degree relative with PCOS
- Obesity
- Type 1, type 2 diabetes, or GDM history
- Signs of insulin resistance / metabolic syndrome
- Premature adrenarche
- Women on antiepileptic drugs (especially valproate)
- Anovulatory infertility
-
Q. Who first described PCOS?
- Stein and Levinthal
-
Q. What is the most common source of androgens in PCOS?
- It is mainly ovarian hyperandrogenism
-
**Pathogenesis **
-
Q. Summarize the pathogenesis of PCOS with a picture?
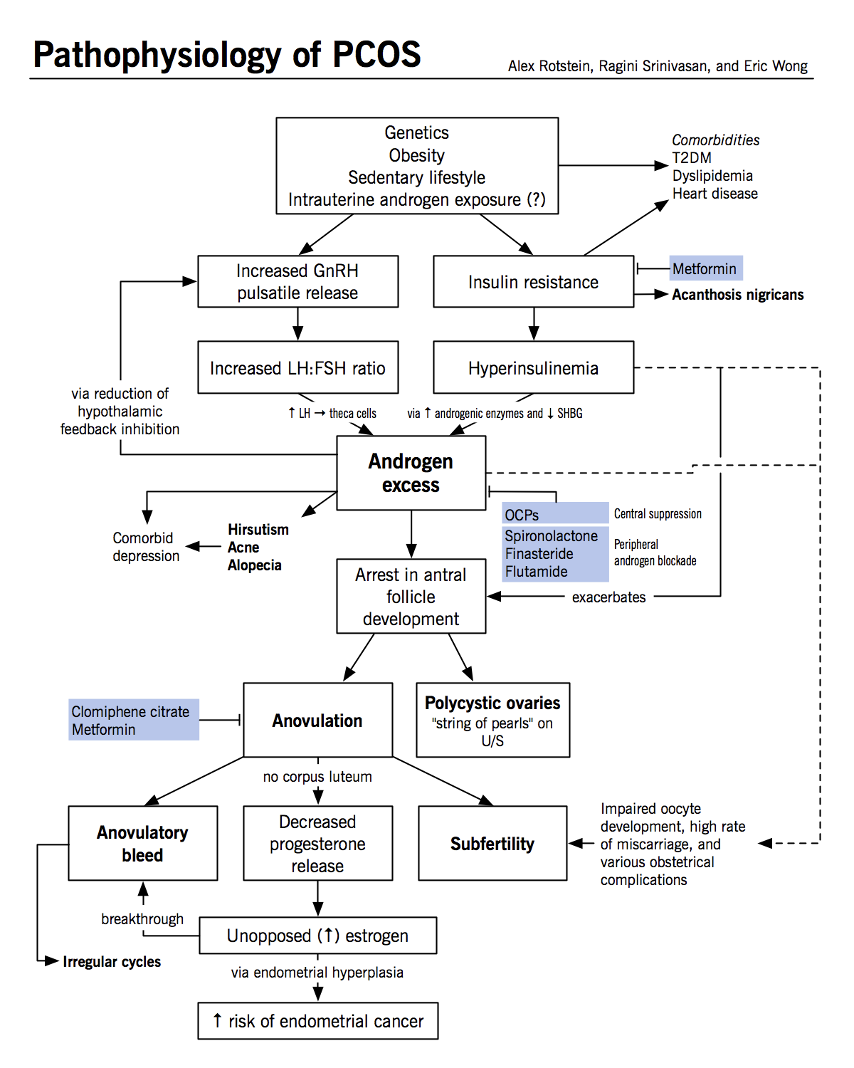
- Ref: Witchel SF, Oberfield SE, Peña AS. Polycystic ovary syndrome: pathophysiology, presentation, and treatment with emphasis on adolescent girls. Journal of the Endocrine Society. 2019 Aug;3(8):1545-73.
-
Q. Does PCOS have a heritable component?
- Yes
- Proven in Twin studies
- The genetic component may be as high as 70% contributing to PCOS
-
Q. What factors contribute to the genetic component of PCOS?
- Difference in energy metabolism
- Difference in gonadotropin secretion- LH predominance
- Difference in secretion/action of insulin
- Difference in androgen biosynthesis by the ovary
-
Q. Which are the candidate genes for PCOS?
- There are 100s of genes implicated
- But two genes which have the strongest evidence-based on GWAS are
- THADA gene
- DENND1A
-
Q. When does GnRH stimulate LH, and when does it stimulate FSH release?
- More rapid GnRH pulse produces LH, and slower GnRH pulse produces FSH
-
Q. What is the LH pulse frequency at various phases of the menstrual cycle?
- Early follicular- 90 min
- Late follicular (close of ovulation)- 60 min
- Early luteal – 100 min
- Late luteal – 200 min
-
Q. What happens in PCOS in terms of GnRH pulse, and what is its consequence?
- There is rapid GnRH release leading to predominant LH production in preference to FSH
- Increase LH Theca cells have LH receptors so increase activation of Theca cell→ theca cells produce androgen so increase ovarian androgen production
- Reduce FSH granulosa cell have FSH receptor → reduced ovarian follicular development
-
Q. Is this the only problem?
- Not all women with PCOS have LH predominant response
- Hence rapid LH pulsation is not the only reason for PCOS, and other things also have to be considered
-
Q. Which drugs reduce insulin resistance?
- Metformin
- TZD
- D-Chiro-Inositol
-
Q. How does insulin contribute to the pathogenesis of PCOS?
- Reduces SHBG
- Theca cells have insulin receptor-activated → androgen production
-
Q. What percentage of women with PCOS have insulin resistance?
- 50-70%
-
Q. Which molecular defect in PCOS links PCOS with diabetes?
- There is a defect in serine phosphorylation
- Abnormal serine phosphorylation in Insulin receptor increase hyperinsulinemia
- Abnormal serine phosphorylation in 17 alpha-hydroxylase (CYP17) → increase ovarian androgen production
-
Q. What is the change in micro RNA seen in PCOS?
- Increase of miR-93 RNA expression
- This may contribute to the insulin resistance
-
Q. Does weight gain contribute to PCOS or vice versa?
- It could be either or both
-
Q. What are some other factors implicated?
- Role of Adrenal androgens
- Role of Diet androgenic content in the diet
- Role of androgen exposure to the fetus during intrauterine life
-
Q. Summarize the various factors involved in the pathogenesis of PCOS
- Genetic component- DENND1A and THADA
- Role of GnRH pulsatility and LH predominance
- Role of insulin resistance
- Role of obesity
- Role of other factors- adrenal androgen, diet, prenatal exposure to androgens
-
Steroid hormone metabolism in polycystic ovary syndrome
-
Q. What are the sources of various androgens in women?
- DHEA/DHEAS- 100% from the Adrenal gland
- Androstenedione- 50% from the ovary and 50% from adrenal
- Testosterone- 25% - ovary, 25% adrenal, 50% from peripheral conversion of androstenadione
-
Q. What is the difference in androgen source in normal premenopausal women vs. women with PCOS?
- In normal premenopausal women, androstenedione and testosterone come 50,50% from the adrenal and ovary
- In PCOS- they come mainly from ovaries instead of adrenals
-
Q. Which product is an exclusive marker of peripheral androgen action?
- Androstanediol
- It is an indicator of androgen action on the skin and hence correlates well with hirsutism
- It is derived from the metabolism of DHT
-
Q. What happens to estrogen levels in PCOS women?
- Estrogen, especially estradiol levels, are normal in women with PCOS
- Estrone derived from androstenedione may be a little higher
-
Q. Do statins reduce hyperandrogenemia by reducing the cholesterol substrate?
- Yes
- Statins can potentially reduce androgen levels in PCOS women by reducing the cholesterol available as substrate
-
- Remember Theca cells have LH receptors and produce androstenedione
- Granulosa cells have FSH receptors and produce estrogen
-
Q. What is the functional classification of PCOS based on the source of androgens?
- Typical PCOS
- Functional ovarian hyperandrogenism
- Increase 17 OHP in response to GnRH analog (basically this is hyper-responsiveness to LH)
- This is seen in 2/3rd of cases
- Atypical PCOS
- Functional ovarian hyperandrogenism with no increase of 17 OHP to GnRH
- Functional adrenal hyperandrogenism
- Hyperandrogenism from neither adrenal nor ovarian source
- Typical PCOS
-
Q. Which are the various tests done to find the source of androgen in PCOS?
- GnRH agonsit test - 17 OHP - >152 ng/dl – s/o of Funtional ovarian hyperandrogenism
- HCG stimulation test- 17 OHP - >152 ng/dl – s/o of Funtional ovarian hyperandrogenism
- Short dexamethasone suppression test- testosterone >26 ng/dl – suggestive of the ovarian source of androgen
- ACTH stimulation test – DHEA – 1500 ug/dl – s/o of Functional adrenal hyperandrogenism