Support us:
- Support us by purchasing our book - Click here for more details: Volume 1- THE BEST OF NOTES IN ENDOCRINOLOGY BOOK SERIES
- Support you by Becoming a YouTube member (Click here)
Connected notes;
- Overview of the management of diabetic kidney disease
- Finerenone for Diabetic kidney disease
- Management of Diabetes in patients with CKD
Video lecture
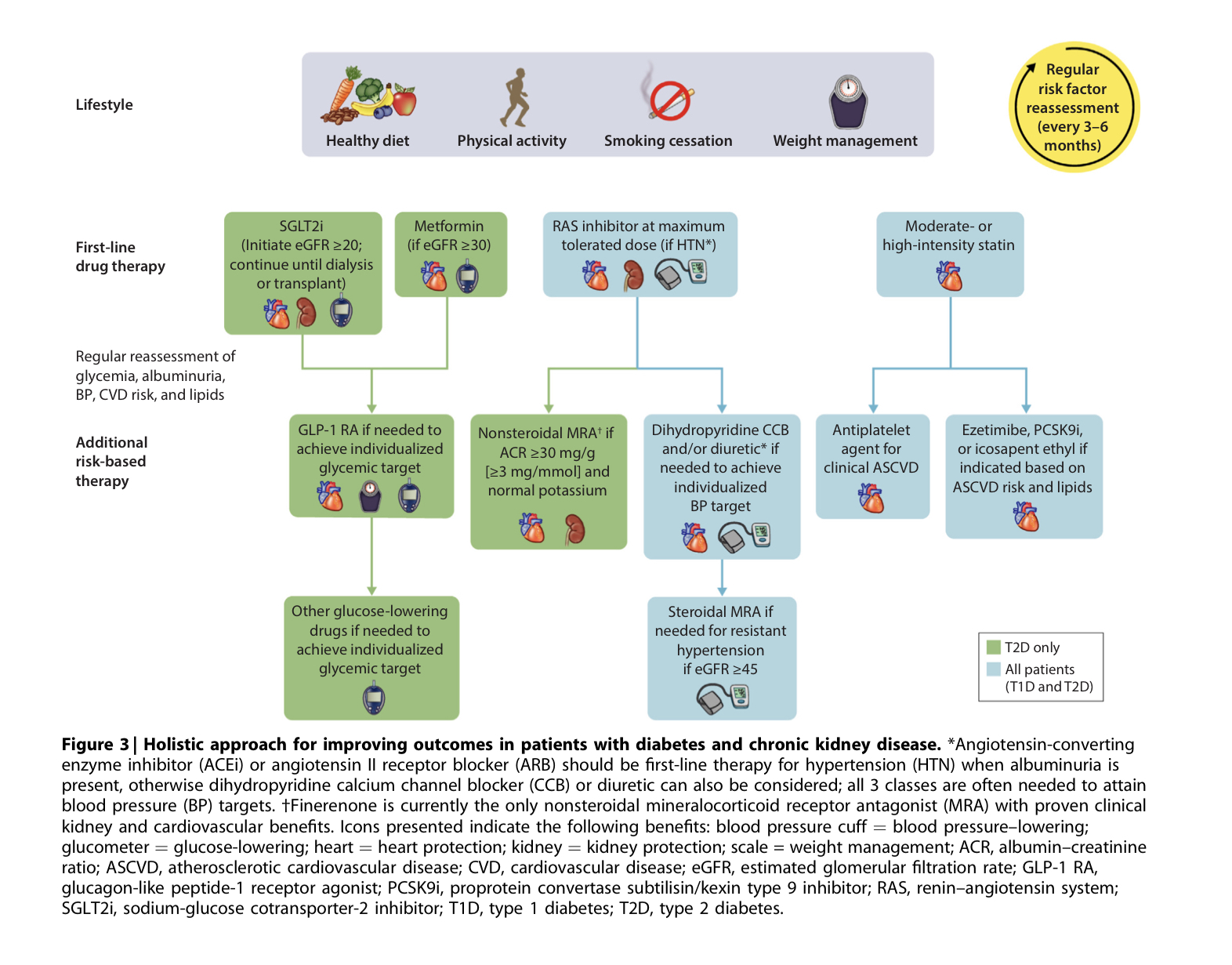
- Q. Summarize the management of Diabetic kidney disease as per the new guidelines.
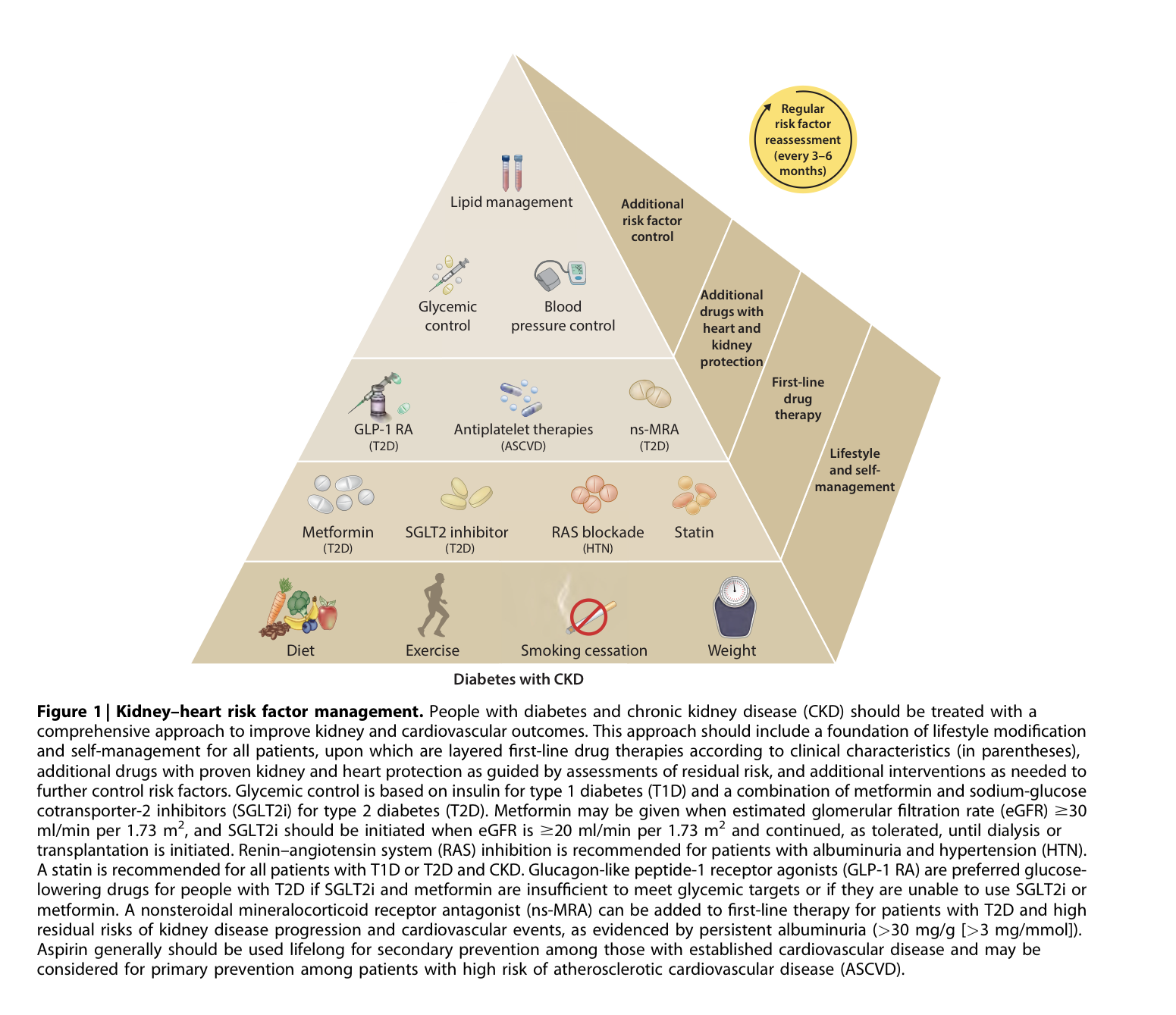
- Q. Give the components of the DKD management pyramid as per the current guidelines.
- Q. Which drugs are considered first-line therapy for the management of patients with Diabetic kidney disease?
-
- Metformin
-
- SGLT2i
-
- RAS blockade
-
- Statin
-
- Q. Which drugs are considered second-line therapy for Diabetic kidney disease?
- GLP-1 RA
- Anti-platelet drugs
- non steroidal Mineralocorticoid receptor agonist - Finerenone
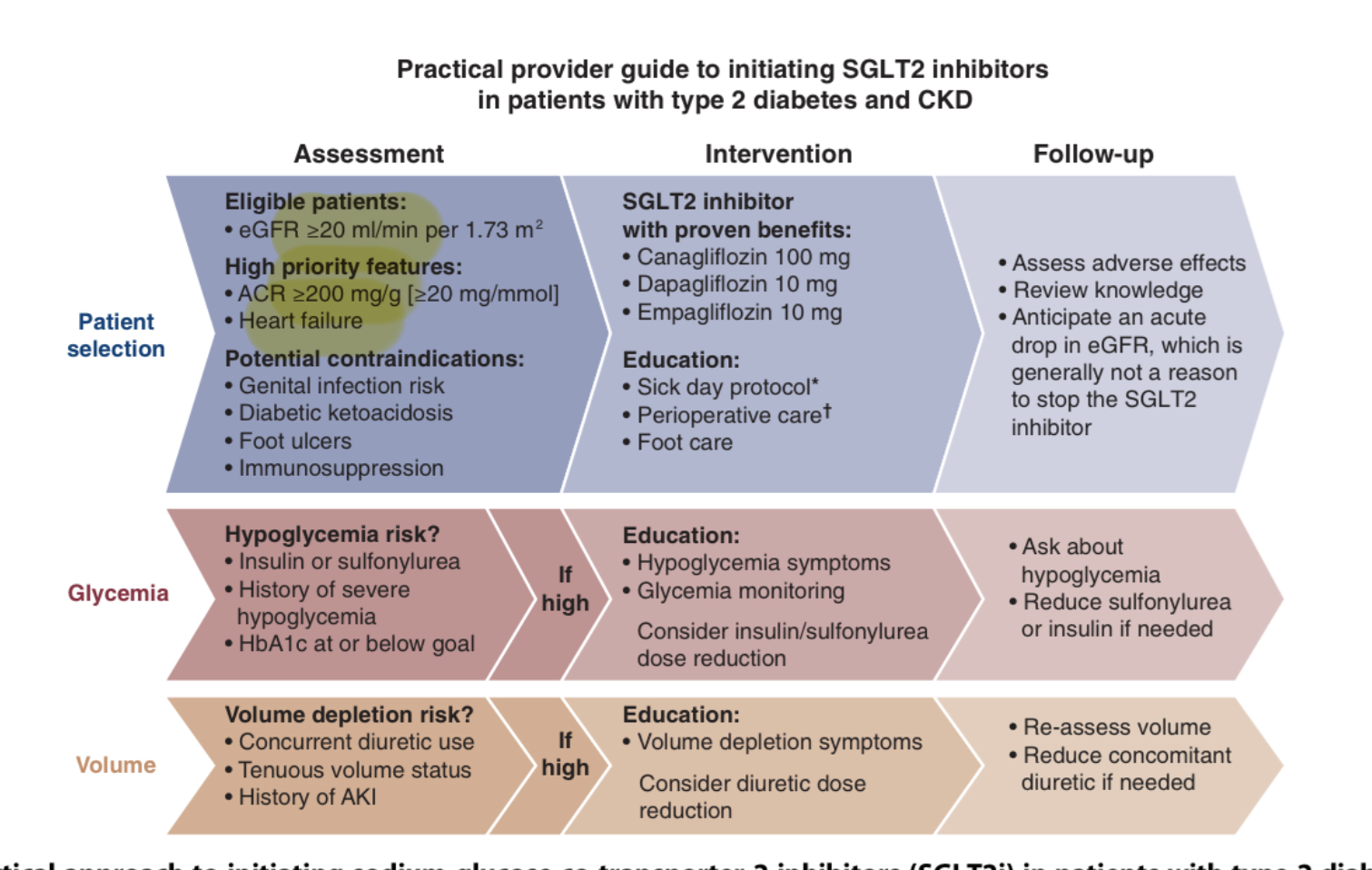
- Q. As per the new guidelines up to what eGFR category can the SGLT2i be used?
- SGLT2i can be used initiated up to eGFR >20
- However, the drug can be continued in patients with type 2 diabetes, if the eGFR falls below this level
- The only consideration for stopping this drug is when the patient requires dialysis
- Q. Which patients with diabetic kidney disease should not be given SGLT2i?
- There is not enough data for:
-
- Type 1 diabetes
-
- Post-renal transplant
-
- Patients on dialysis
-
- eGFR <20
- at this eGFR SGLT2i should NOT be initiated, but if the patient is already on the drug and eGFR falls to this level it can be continued till the patient is started on dialysis
- Q. Summarize some practical recommendations for initiating SGLT2i in Diabetic kidney disease.
- Q. Where does GLP-1 receptor agonist stand in the equation?
- It is considered the preferred second-line therapy in patients with Diabetic kidney disease for diabetes control, CV risk reduction, and weight loss
- However, since it does not have a dedicated CKD trial, it misses out on Level A evidence
- Q. What are the indications for Finerenone as per the current guideline?
-
- Type 2 diabetes
-
- eGFR- >25
-
- UACR >30
-
- On maximum dose of RAAS blocker
-
- Baseline potassium <4.8 (with caution up to <5.0)
-
- Q. Which is another non-steroidal mineralocorticoid receptor agonist other than Finerenone under trial?
- Esaxerenone
- Q. Can Finerenone be used with SGLT2i ?
- The benefit of the two seems complimentary
- Also it seems SGLT2i mitigates the risk of hypokalemia in these patients
- Q. In which cases is steroidal mineralocorticoid receptor agonist (eg: Spironolactone ) suggested?
- If the patient has Heart failure and Primary Aldosteronism
- In these cases, steroidal MRA is preferred over non-steroidal because of its proven benefits in these conditions
Ref: Rossing P, Caramori ML, Chan JCN, Heerspink HJL, Hurst C, Khunti K, Liew A, Michos ED, Navaneethan SD, Olowu WA, Sadusky T, Tandon N, Tuttle KR, Wanner C, Wilkens KG, Zoungas S, Craig JC, Tunnicliffe DJ, Tonelli MA, Cheung M, Earley A, de Boer IH. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease: an update based on rapidly emerging new evidence. Kidney Int. 2022 Nov;102(5):990-999. doi: 10.1016/j.kint.2022.06.013. PMID: 36272755.