- Credits
- Section Writer: Dr. Om J Lakhani
- Section Editor: Dr. Om J Lakhani
Support us:
- Support us by purchasing our book - Click here for more details: Volume 1- THE BEST OF NOTES IN ENDOCRINOLOGY BOOK SERIES
- Support you by Becoming a YouTube member (Click here)
Reference: Buzzetti et al[1]
-
Q. What are the diagnostic criteria for Latent autoimmune diabetes of Adulthood (LADA) ?
- Age > 30 year
- At least 1 insulin cell autoantibodies positive
- Period of 6 months on insulin independence
-
Q. What are the expanded clinical criteria for Latent autoimmune diabetes of Adulthood (LADA) ?
- Age at onset > 30 years
- A family or personal history of autoimmunity
- A reduced frequency of metabolic syndrome compared with people with full-on type 2 diabetes: lower HOMA, lower body mass index, lower blood pressure, normal HDL compared with people with type 2 diabetes
- No disease-specific difference in cardiovascular outcomes between these patients and those with type 2 diabetes
- C-peptide levels fall more slowly than in traditional type 1 diabetes
- Positivity for anti-GAD antibodies is the most sensitive marker, but other autoantibodies can be found as well, just less frequently
- Non–insulin-requiring at the onset
-
Q. Which is the preferred marker to diagnose LADA?
- Anti GAD65
-
Q. What are the subtypes of LADA?
- LADA1 – lesser C peptide, more ketosis-prone, higher GAD antibody
- LADA2- greater C peptide, less ketosis-prone, lesser GAD antibody positivity
-
Q. What is LADY?
- Latent autoimmune diabetes in Young
- Similar to LADA but age is <30 years
-
Q. What is the importance of a positive GAD antibody in any diabetic individual?
- Positive GAD antibody in any diabetic predicts the requirement for early insulin requirement
-
Q. Which is the latest antibody for Type 1 Diabetes or Latent autoimmune diabetes of Adulthood (LADA) ?
- Tetraspanin 7
-
Q. Are there any benefits of early insulin initiation?
- Yes
- Early insulin initiation would help give rest to beta-cell and give overall good control
-
Q. Which heat shock protein has been found to reduce beta-cell destruction?
- Diapep 277- a heat shock protein 60 derivative has been found to reduce the incidence of beta-cell destruction in both type 1 diabetes and LADA
-
Q. What vaccine has been found to retard beta-cell damage?
- Anti GAD65 vaccine – DIAMYD
-
Q. How do these vaccines work?
- They cause a shift from pro-inflammatory Th1 cells to anti-inflammatory Th2 cells
- This shift suppresses the cytokine produced by Th1
- This is a form of “acquired immune tolerance”
-
Q. What is the core difference between adult type 1 diabetes and LADA?
- The core difference is the speed of the beta-cell destruction leading to the dependency on insulin
- Adult-onset Type 1 Diabetes have more rapid beta-cell destruction unlike LADA
- This is differentiated by the criteria which say 6 or more months of insulin independence after onset which is required for LADA
- If insulin requirement is before 6 months - it is adult type 1
- otherwise, it is LADA
-
Q. Which OAD must be avoided for use in LADA?
- Avoid sulphonylurea
-
Q. Can other OAD be used in LADA?
- Yes
- There are small studies for benefit of all other OADs including SGLT2i in LADA patients
-
Q. Should all patients with Type 2 Diabetes mellitus be screened for LADA?
- Yes
- According to the recent guidelines on the topic
-
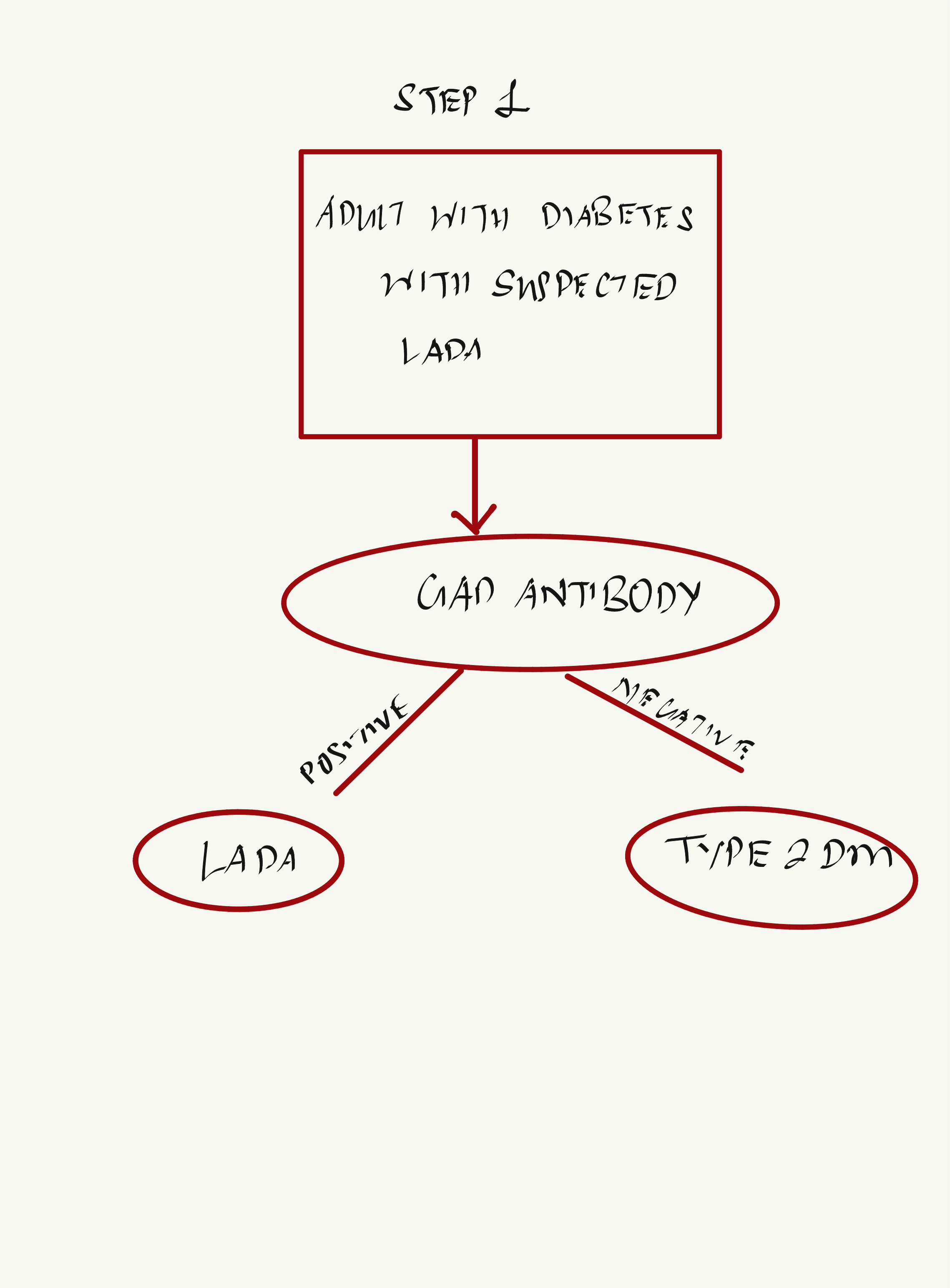
Q. Give the algorithm for diagnosis and management of Latent autoimmune diabetes of Adulthood (LADA)
-
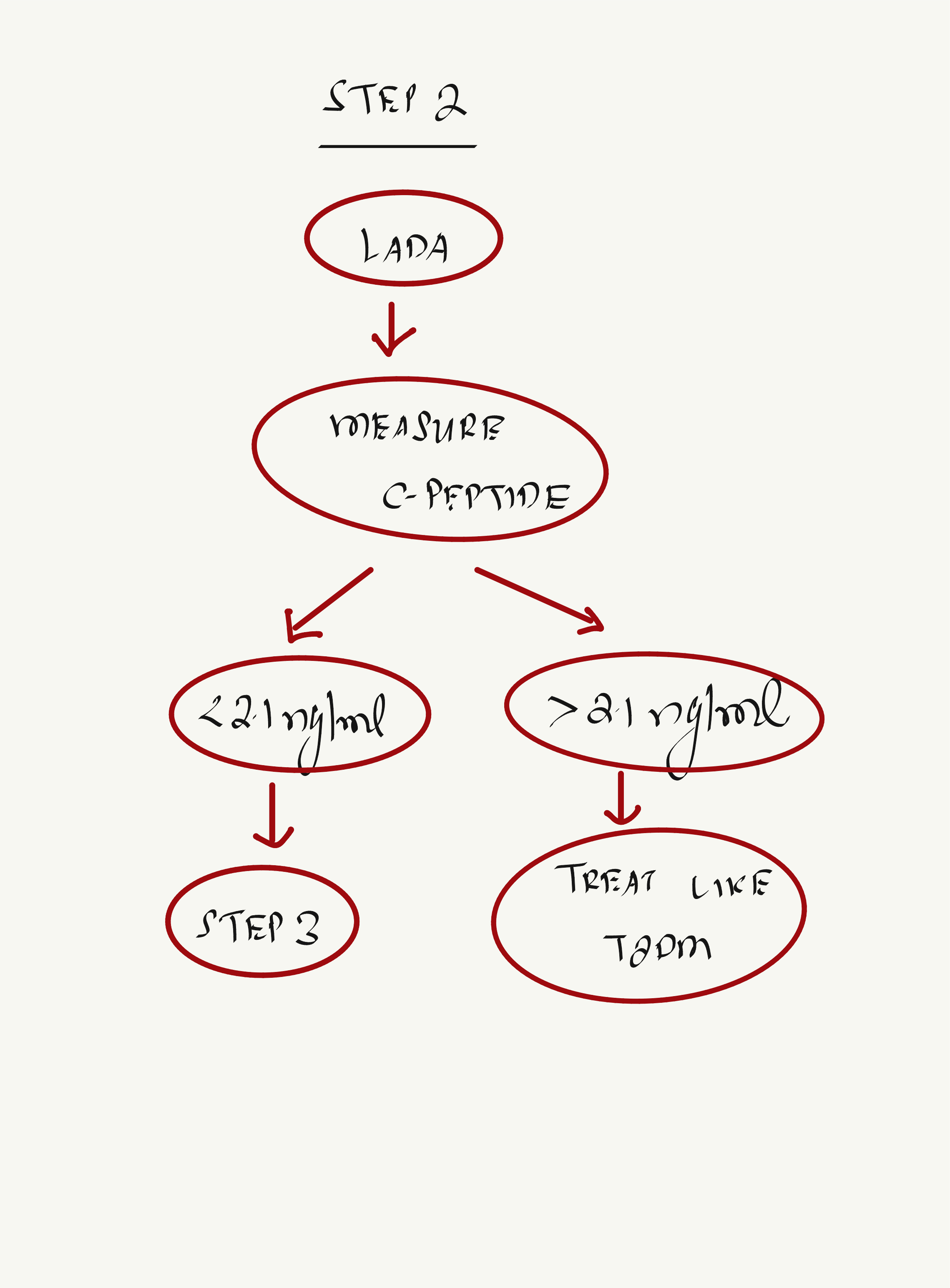
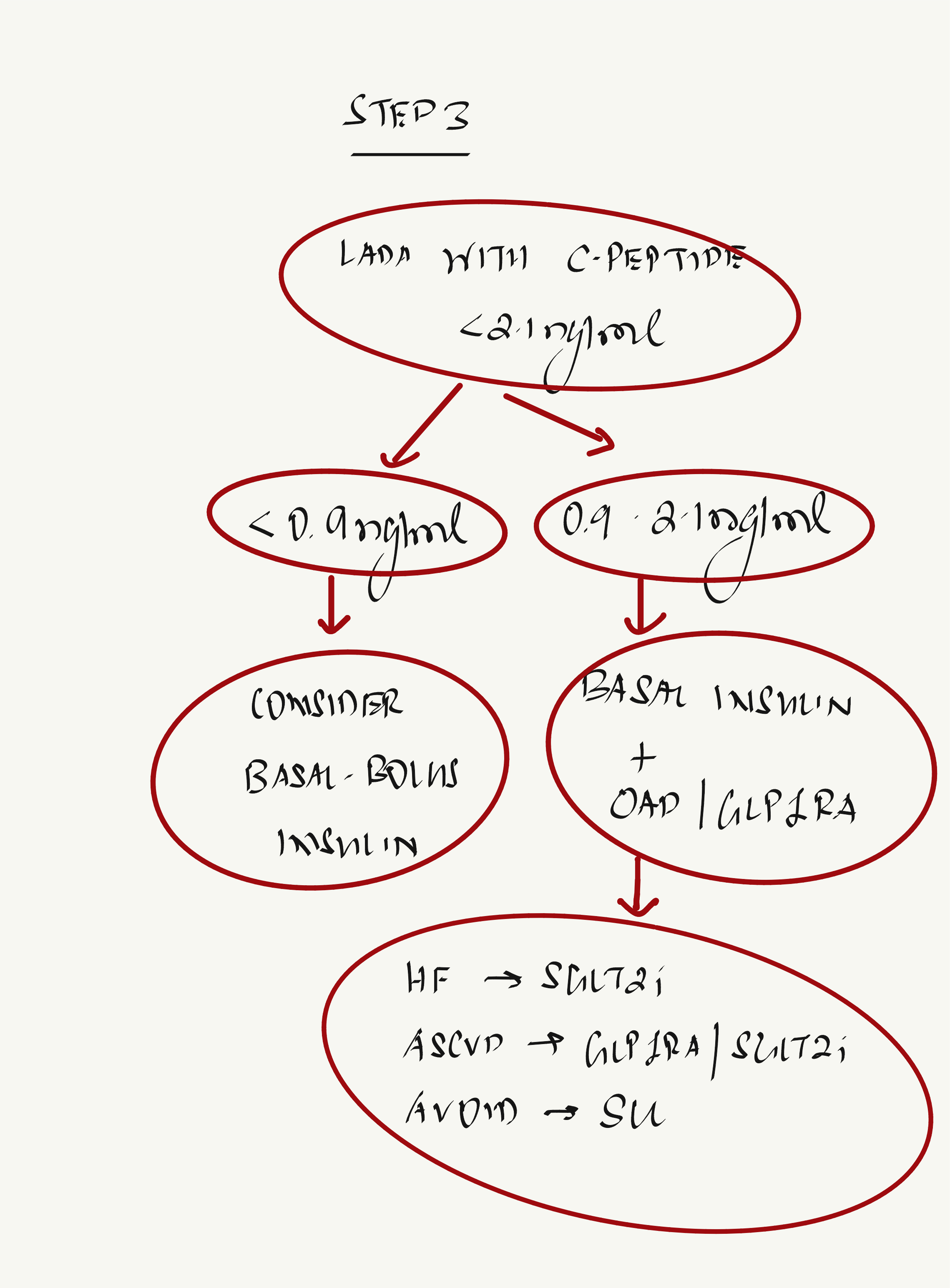
Q. What is the C-peptide-based approach to the management of a patient with LADA?
- C-peptide
- <0.9 ng/ml (0.3 nmol/l) - Patient should be on basal bolus insulin
- 0.9-2.1 ng/ml (0.3-0.7 nmol/l) - Patient should be on basal insulin plus OAD
- More than 2.1 ng/ml (>0.7 nmol/l) - treat with OAD and/or as per the ADA guidelines for type 2 diabetes
- C-peptide
-
Q. What should be the glucose levels while performing the C-peptide assay?
- 80-180 mg/dl
-
Q. Apart from the insulin requirement and OAD, which other factors must be kept in mind when a patient has LADA instead of Type 2 Diabetes mellitus ?
- Increased risk of other autoimmune diseases - including hypothyroidism
14-Aug-2023, #update
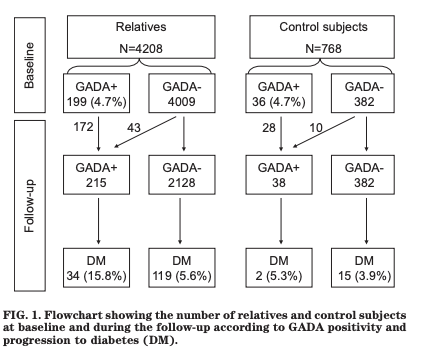
- Q. What were the conclusion from the Botnia study group published in 2010 ?
- The study was done to look at the impact of GAD antibody in the future risk of diabetes in non diabetic individuals
- The study found the the following:
- • GADA positivity is a strong predictor of diabetes, regardless of family history.
- • People with high GADA concentrations are at an increased risk of developing diabetes.
- • GADA positivity tends to occur in families with type 1 diabetes or latent autoimmune diabetes in adults.
- • Low or medium levels of GADA do not impact the incidence of diabetes in individuals without a family history of diabetes.
- • Elevated GADA concentrations indicate an increased risk of diabetes in both relatives and control subjects.
- • The risk of diabetes is influenced by age, sex, BMI, GADAs, and family history of type 1 or type 2 diabetes.
- • GADA positivity significantly raises the risk of diabetes, in addition to traditional risk factors for type 2 diabetes
- This flow chart summarizes this well:
- Ref: Lundgren VM, Isomaa B, Lyssenko V, Laurila E, Korhonen P, Groop LC, Tuomi T, Botnia Study Group. GAD antibody positivity predicts type 2 diabetes in an adult population. Diabetes. 2010 Feb 1;59(2):416-22.
- Q. What level of GAD65 antibody was considered as positive in this study ?
- Levels about 32 IU/l were considered positive
- Q. Should patients with LADA be given SU ? Does it impact long term beta-cell reserve ?
- A study published in JCEM concluded that it is better to give insulin early and not Sulphonylurea in patients with LADA
- Study conducted by Taro Maruyama et al. that focused on comparing the effectiveness of insulin therapy versus sulfonylurea (SU) treatment in preserving or reversing beta-cell function in patients with slowly progressive insulin-dependent diabetes or LADA.
- The study was a randomized clinical trial that included 60 patients with a 5-year duration or shorter of diabetes.
- The primary endpoint of the study was an insulin-dependent state defined by low levels of serum C-peptide values.
- The results showed that the progression rate to an insulin-dependent state was lower in the insulin group compared to the SU group, indicating that insulin therapy may be more effective in preserving beta-cell function in LADA patients.
- Ref: Maruyama T, Tanaka S, Shimada A, Funae O, Kasuga A, Kanatsuka A, Takei I, Yamada S, Harii N, Shimura H, Kobayashi T. Insulin intervention in slowly progressive insulin-dependent (type 1) diabetes mellitus. The Journal of Clinical Endocrinology & Metabolism. 2008 Jun 1;93(6):2115-21.
Buzzetti R, Tuomi T, Mauricio D, Pietropaolo M, Zhou Z, Pozzilli P, Leslie RD. Management of Latent Autoimmune Diabetes in Adults: A Consensus Statement From an International Expert Panel. Diabetes. 2020 Oct;69(10):2037-2047. doi: 10.2337/dbi20-0017. Epub 2020 Aug 26. PMID: 32847960; PMCID: PMC7809717. ↩︎